Chronic bronchitis is one of the most common chronic respiratory diseases. The main cause is smoking. Typical symptom is chronic cough with sputum. In severe cases, respiratory distress is added. Chronic bronchitis affects the majority of male smokers. Read everything important about symptoms, causes, treatment and dangers of chronic bronchitis!

Chronic bronchitis: description
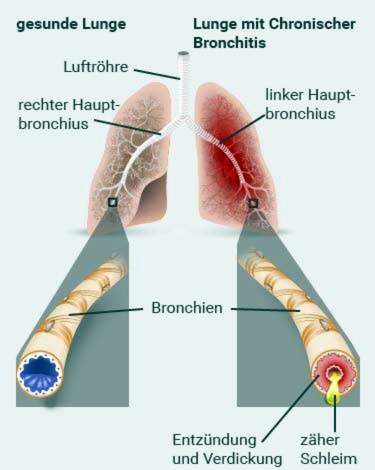
Doctors call a bronchitis chronic if someone suffers from coughing with sputum almost every day for at least three months for two consecutive years. In those affected the mucous membrane of the bronchi is chronically inflamed. (The bronchi are large branches of the trachea in the thorax.)
There are two types of chronic bronchitis:
- simple (non-obstructive) chronic bronchitis: Here, the bronchi are chronically inflamed. It is usually the lighter of the two forms of disease.
- obstructive chronic bronchitis: Here the chronic inflamed bronchi are additionally constricted (obstruction = obstruction, blockage). One also speaks of chronic obstructive bronchitis (COB) or – popularly – of “smoker’s cough”.
Obstructive chronic bronchitis can develop into one chronic obstructive pulmonary disease(COPD). Then the alveoli are also over-inflated (pulmonary emphysema). COPD is therefore a chronic obstructive bronchitis in combination with pulmonary emphysema. The disease is one of the leading causes of death worldwide and also in Germany.
Who is affected by chronic bronchitis?
In Germany, about 10 to 15 percent of adults have a simple chronic bronchitis. Smoking is the most important risk factor: every second smoker over the age of 40 has chronic bronchitis. Men get sick much more often than women.
Obstructive chronic bronchitis affects about two to three percent of women and four to six percent of men. Almost all patients have smoked or continue to do so even after the diagnosis.
Chronic bronchitis: symptoms
Chronic bronchitis goes with productive cough (Cough with expectoration). Especially in the morning he makes himself felt. Usually that is Expectoration slimy-whitish, If bacteria have spread on the inflamed bronchial mucosa, the discolorates Expectoration yellowish-purulent.
If the chronically inflamed bronchi are additionally irritated (eg by air pollutants, tobacco smoke, infections, etc.), the symptoms can get worse.
Note: Coughing with more or less sputum is also the typical sign of acute bronchitis. In chronic bronchitis, however, the symptoms are significantly less pronounced.
The general condition of the patient is usually good for chronic bronchitis. Problems with breathing do not occur.
In the further course a simple chronic bronchitis can become one chronic obstructive bronchitis evolve, that is, the inflamed bronchi narrow increasingly. This hinders the passage of air during inhalation and exhalation.
At a slight narrowing occurs only under stress breathlessness on, for example while running. As the disease progresses, the airways contract more and more. This makes breathing harder and harder. Even with moderate effort (such as climbing stairs), patients quickly get out of breath. In the worst case causes obstructive chronic bronchitis Shortness of breath even without physical effort (in peace).
The difficult breathing costs the patient a lot of energy. They are therefore only less powerful.
The most important complication of obstructive chronic bronchitis may be one Overload of the right heart (Cor pulmonale) develop. In the consequence can Arrhythmia occur. Due to the reduced pumping power of the heart muscle, water accumulates in the tissue of the legs (edema). In addition, sufferers constantly suffer from a significant lack of oxygen. Bluish lips and fingernails are signs of this.
Obstructive chronic bronchitis can cause pulmonary emphysema symptoms at all stages. By overstretching and destroying the alveoli, the respiratory effort of the lungs decreases permanently. The lungs are over-inflated. Chronic bronchitis has caused COPD. The transition is flowing.
Caution: Chronic bronchitis affects the self-cleaning capacity of the lungs. Patients are therefore prone to additional bacterial respiratory infections. The risk of pneumonia is also increased.
Chronic bronchitis: causes and risk factors
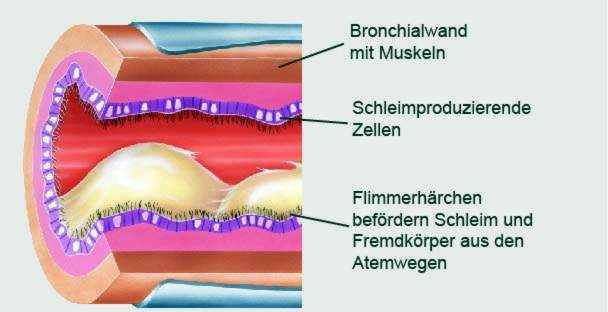
Chronic bronchitis is primarily a “smoking disease”: tobacco smoke directly damages the mucous membrane of the respiratory tract. It inflames and produces more viscous mucus.
In addition, tobacco smoke inhibits the movement of cilia in the bronchi. These normally carry mucus, germs and other foreign substances towards the exit (trachea and throat). For smokers, they are no longer capable of doing so.
The combination of increased mucus production and impaired removal of mucus is typical for chronic bronchitis.
Rarer causes of chronic bronchitis
Rarely solve pollutants Chronic bronchitis in the environment and in the workplace. These can be, for example, gases, dusts and vapors that irritate the respiratory tract. Examples are sulfur dioxide, nitrogen oxides, ozone, cadmium, silicates, wood, paper, grain and textile dust.
Also rare is a chronic bronchitis caused by so-called endogenous factors. These are factors that are inherent in the patient, for example genetic factors, For example, the congenital deficiency of the enzyme alpha-1-antitrypsin can cause chronic bronchitis. Even a so-called antibody deficiency syndrome (lack of IgA or IgG) comes as a cause in question. Other people suffer from a congenital disorder of ciliary hairs in the airways. They often develop obstructive chronic bronchitis as early as childhood.
Some patients have one severe acute respiratory infection extended to chronic bronchitis. This danger exists especially when the infection not treated or late becomes. Also repeated respiratory infections can contribute to the development of chronic bronchitis.
Doctors still discuss about other risk factors for (obstructive) chronic bronchitis. These include a low birth weight, early childhood infections, a tendency to allergic diseases (such as eczema, hay fever, allergic asthma) and a hypersensitive respiratory system.
Chronic bronchitis: examinations and diagnosis
Chronic bronchitis should be diagnosed and treated by an experienced family doctor or pulmonologist.
The doctor will first talk extensively with the patient to get his medical history (anamnesis). Possible questions are:
- What symptoms do you have exactly? Since when do the complaints exist?
- Are you a Smoker?
- Since when and how much do you smoke?
- Goods / Are you exposed to a special pollutant load, such as at the workplace?
- Do you have any pre or basic diseases?
Then follows the physical examination, Among other things, the doctor will listen to the lungs with the stethoscope. He usually has rattling noises. If there is an obstructive chronic bronchitis, a so-called wheezing is generally heard. That’s a whistling sound while exhaling. It indicates narrowed airways.
Lung function test
With a pulmonary function test, the doctor can check how well the patient’s lungs are working. This is especially important for obstructive chronic bronchitis. Various methods are available, for example spirometry. More specifically, one can test the lung function with a so-called body plethysmography.
Peak flow measurement may also help to assess the extent of obstructive chronic bronchitis. In addition, repeated peak flow measurements allow the success of a treatment to be assessed. If there is a suspicion that the patient has a hypersensitive bronchial mucosa, methacholine or histamine may be used to provoke a provocation test. For a fine vapor of the active ingredient is inhaled. Then the peak flow meter is used to measure whether the air flow rate has decreased during exhalation.
X-ray examination of the ribcage
X-rays of the chest (chest X-ray) are mainly used to rule out other causes of the symptoms. For example, lung cancer and lung tuberculosis can trigger similar symptoms to chronic bronchitis. The same applies to foreign bodies in the lungs as well as so-called bronchiectasis (outgrowths of the bronchi).
Chronic bronchitis leaves irregular, diffuse streak or band-shade streaks on the radiograph. Physicians speak here of Plattenatelektasen or “dirty chest”. The shadows are caused by the fact that the air sacs contain too little or no air. The corresponding lung area is thereby reduced or not deployed.
Further investigations
Sometimes the ribcage is used by Computed tomography (CT). For example, bronchiectasis can be ruled out.
The doctor can do one Sample of coughed ejection (Sputum) examine more closely. For example, it can be determined whether an additional bacterial infection has spread in the respiratory tract.
Often, too blood gases measured, ie the oxygen and carbon dioxide content and the pH of the blood. From the results it can be estimated how advanced a chronic bronchitis is. This is especially important for obstructive chronic bronchitis.
If the doctor suspects that obstructive chronic bronchitis overburdens the right half of the heart (cor pulmonale), further investigation is needed. These include above all an electrocardiography (ECG) as well as one Ultrasound examination of the heart (Echocardiography). Possibly also an examination by means of cardiac catheterization meaningful.
Chronic bronchitis usually develops only in older age. However, if the patient is younger than 45 years and / or there are cases of COPD in his family, the cause is often an inheritable deficiency of alpha-1-antitrypsin (antirypsin deficiency). Also a congenital lack of certain antibodies (antibody deficiency syndrome) can be behind it. Corresponding information provides a blood test.
Chronic bronchitis: treatment
Smoking is the main cause of chronic bronchitis. The treatment is therefore only successful if the patient completely dispensed with the tobacco. He must also avoid passive smoking. He should also avoid other pollutants that can irritate the bronchi. If the patient comes in contact with such irritants at the workplace, retraining may be advisable.
The other chronic bronchitis therapy depends on the severity of the disease. In principle, there are non-drug and drug treatments.
Non-drug measures
Regardless of the severity of the disease: Chronic bronchitis requires intense Training the patient, This can do much to stop the progression of the disease. He should, for example, learn how to inhaled properly and using a tapping massage fixed mucus in the bronchi can detach.
Meaningful are synonymous special breathing techniques, It is often recommended, for example, the “lip brake”: It tries to exhale through the almost closed lips. This creates a higher pressure in the bronchi, which reduces their collapse. Also one breathing exercises can support the work of breathing. A physiotherapist can show the patient appropriate exercises.
Chronic bronchitis tempts many patients to look after themselves. This is especially true if they also have narrowed airways (obstructive chronic bronchitis). But it is very important for the patients stay physically active, Regular exercise and exercise increase overall resilience and quality of life. If the chronic bronchitis is already advanced, the training should take place under medical supervision.
A healthy, balanced diet is also very important. It generally promotes good health. It is especially important in underweight patients. Above all, obstructive chronic bronchitis can cost so much strength that those concerned lose significantly more weight. Then they should eat a high calorie diet. In general, one should also pay attention to a sufficient hydration.
Chronic bronchitis: medication
If necessary, the doctor prescribes bronchodilator drugs, for example, so-called beta-sympathomimetics. They relieve the respiratory distress that accompanies obstructive chronic bronchitis.
Sometimes patients also receive so-called glucocorticoids (“cortisoneThese inhibit the chronic inflammation in the bronchi and have a decongestant effect on the mucous membrane The active ingredients are usually inhaled.
If the chronic bronchitis is accompanied by a bacterial infection, the doctor prescribes antibiotics.
An (obstructive) chronic bronchitis can worsen acutely (exacerbation). Possible triggers are, for example, acute infections with bacteria or viruses. Then a quick and intensive treatment by the doctor is necessary. If necessary, those affected must be treated in the hospital.
Note: Some patients report that they are good at expectorants (such as acetylcysteine or ambroxol). The effectiveness of these drugs is not scientifically proven.
Chronic bronchitis: course and prognosis
Sometimes a simple chronic bronchitis is curable – provided it is still at a very early stage and the trigger (smoking, other harmful substances, etc.) is strictly avoided. Simple chronic bronchitis can persist for life. Those affected can still get very old – the simple chronic bronchitis does not shorten the lifetime.
In just under 20 percent of patients, over time, obstructive chronic bronchitis develops from the simple. The airways are then permanently constricted. With drugs (such as sympathomimetics), this narrowing can only be partially reversed.
If, in addition to obstructive chronic bronchitis, hyperinflation of the alveoli (pulmonary emphysema) develops, medical experts speak of one chronic obstructive pulmonary disease (COPD). This is a very serious and progressive lung disease. It shortens the life expectancy of a patient by about eight to ten years.
Another dreaded complication is the Right heart failure (cor pulmonale).
In addition, chronic bronchitis is generally more susceptible to infections, such as influenza and pneumonia. Such complications can significantly worsen the condition of a patient. Therefore, people who have obstructive chronic bronchitis should be regularly vaccinated against the flu and pneumococci (common causes of pneumonia).
Additional information:
guidelines:
- Guideline “Diagnosis and Therapy of Adult Patients with Acute and Chronic Cough” of the German Society for Pulmonology (as of 2015)