Angina pectoris (medical stenocardia) means chest tightness. It manifests itself in a sudden pain in the heart and a feeling of pressure in the chest. The angina pectoris is triggered by a lack of oxygen in the heart. There is danger to life, so you should call the emergency doctor immediately! Angina pectoris is usually treated well with medication. Learn, among other things, how the symptoms differ between men and women and what you can do to prevent angina.

Quick Overview
- What is angina pectoris? Sudden, painful chest tightness
- symptoms: Pain behind the sternum, which can radiate, u. a. also shortness of breath, nausea, feeling of tightness in the throat, numbness and anxiety, in women / the elderly: tiredness, shortness of breath
- Causes: inadequate supply of the heart with oxygen-rich blood (mostly due to coronary heart disease, CHD)
- Risk factors: Smoking, high blood pressure, diabetes mellitus, older age
- Treatment: Medicines (in particular nitro preparations); possibly surgery
- Forecast: Angina may be severe, including fatal heart attacks. Therefore, it must necessarily be treated. Also important are general measures such as exercise and healthy eating to reduce the risk of seizure.
Angina: Symptoms & Warning Signs
Doctors refer to angina pectoris (chest tightness, heart disease, stenocardia) paroxysmal pain behind the sternum, It is usually the main symptom of arteriosclerosis of the coronary arteries (coronary heart disease = coronary heart disease). Angina pectoris is actually a symptom and not a disease.
Depending on the course, doctors distinguish between stable and unstable angina pectoris.
General angina pectoris symptoms
An angina pectoris usually expresses itself with sudden pain and a Feeling of tightness, burning sensation, pressure or anxiety behind the breastbone, The pain often radiates to other parts of the body, such as the neck, neck, lower jaw, teeth, arms or upper abdomen. In addition, pain may occur between the shoulder blades.
Affected also often describe Severity and numbness in arm, shoulder, elbow or hand. This mostly affects the left side of the body. In addition, symptoms such as sudden difficulty in breathing, nausea, Vomit, sweats and a oppressive, choking feeling in the throat occur. These signs are often accompanied by anxiety to death and suffocation fear.
Special features of women
In women, angina pectoris usually has other symptoms than men: symptoms such as tiredness, shortness of breath and stomach upset are the typical signs here. The classic chest pain, however, occurs only in a few women.
Special features of the elderly
Older patients (especially those over the age of 75) often show symptoms similar to those of angina pectoris. In a seizure, they often complain of shortness of breath and a performance kink.
Special features of diabetes
Angina pectoris in diabetes (diabetes) has a peculiarity: Patients with diabetes-related nerve damage (diabetic polyneuropathy) often feel no pain, because pain stimuli can no longer be fully transmitted by the damaged nerves. The angina pectoris can therefore be almost painless (mute) in diabetics or accompanied by only minor pain.
Stable angina pectoris: symptoms
In stable angina pectoris, the attacks of angina pectoris are relatively similar each time. The signs of chest tightness are triggered by some form of stress. This can be a physical or emotional strain, cold or an extensive meal. The pain can radiate down to the neck, lower jaw, teeth, shoulder and arms. The symptoms usually go away within 15 to 20 minutes. If you apply a nitrospray for the signs of angina pectoris, they will stop sounding after about five minutes.
Stable angina pectoris is classified into five stages according to the Canadian Cardiovascular Society:
|
stage |
complaints |
|
0 |
No symptoms. |
|
I |
No complaints with everyday stress, but with sudden or prolonged exposure. |
|
II |
Complaints in case of stronger effort. Normal physical stress is little restricted. |
|
III |
Complaints with easier physical stress. |
|
IV |
Resting and complaints with the least physical stress. |
Unstable Angina: Symptoms
Unstable angina pectoris refers to various forms of chest tightness with non-constant symptoms. For example, the seizures may become stronger or longer from time to time. Or they also occur at rest or even at low load. Rest or previously effective drugs (such as nitrospray) hardly help here against the symptoms.
A special form of unstable angina pectoris is the rare Prinzmetal’s angina. Here the heart disease vessels (med. Coronary vascular spasm) become cramped. It occurs in peace, for example while asleep.
An unstable angina pectoris can develop from a stable chest tightness or occur out of nowhere.
The unstable angina pectoris is divided into three degrees of severity:
|
class |
severity |
|
I |
New onset severe or increasing angina pectoris |
|
II |
Angina at rest within the last month, but not in the last 48 hours |
|
III |
Angina pectoris at rest within the last 48 hours |
In unstable angina, there is a high risk of heart attack (20 percent). Therefore, the emergency doctor must be called immediately in a seizure! Incidentally, meizins speak of acute coronary syndrome when unstable angina pectoris becomes a heart attack.
Angina pectoris: causes and risk factors
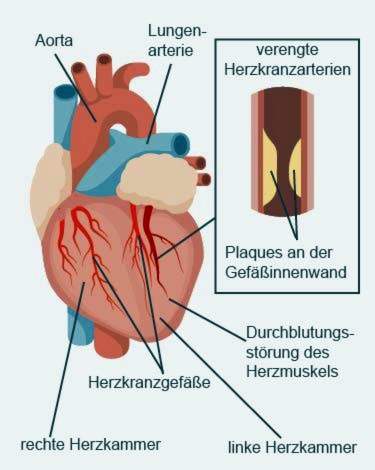
If the cardiac muscle is insufficiently supplied with blood like an attack, it causes angina pectoris. Cause is usually a narrowing of the vessels as a result of hardening of the arteries (Arteriosclerosis) of the coronary arteries. Rarely does an anginal attack happen through Spasms of the vessels (Vasospasms), such as Prinzmetal’s angina.
In arteriosclerosis – the main cause of angina pectoris – the blood vessels are narrowed by deposited fats, platelets, connective tissue and lime. If the heart-supplying vessels (coronary arteries) affected by it, the heart receives too little oxygen and nutrients. Doctors then speak of one Coronary heart disease (CHD) with the main symptom angina pectoris.
Risk factors such as smoking, increased blood pressure, diabetes mellitus (diabetes) and old age favor the deposition of blood lipids on the arterial walls. By inflammatory processes, the wall of the blood vessel transforms – it produces an arteriosclerotic (atheroskelrotic) plaque. For many years, the vessels harden and their diameter gets smaller and smaller. When such a plaque ruptures in the coronary vessels, blood clots form on the spot, which can completely occlude the artery.
If the heart muscle area, which supplies this artery, is no longer supplied with blood and dies, it is called a myocardial infarction.
The following factors increase the risk of arteriosclerosis of the coronary arteries (CHD):
- Nutrition: High-fat and high-calorie foods lead in the long term to obesity and high cholesterol levels.
- overweight
- lack of exercise
- male gender: Men have a higher atherosclerosis risk than menopausal women. The latter are protected by the female sex hormones (estrogen). After the menopause with the stop of estrogen production, this protective effect is lost.
- genetic predisposition: In some families cardiovascular diseases like KHK are more common, so the genes seem to play a role. The risk is increased if first-degree relatives before the age of 55 (women) or before the age of 65 (men) have CHD.
- Smoke: Among other things, substances in tobacco smoke promote the formation of unstable plaques in the vessels.
- High blood pressure: Increased blood pressure values directly damage the inner walls of the vessel.
- elevated cholesterol levels: High LDL cholesterol and low HDL cholesterol promote plaque formation.
- Diabetes mellitus: If the diabetes is poor, the blood sugar is permanently too high, which damages the blood vessels.
- increased inflammatory values: e.g. an increased CRP level in the blood (makes the plaques unstable).
- higher age: With age, the risk of arteriosclerosis of the coronary arteries increases,
Angina: Treatment
The primary goal of angina pectoris treatment is to prevent severe seizures and heart attacks. The risk of infarction exists especially in unstable angina pectoris. This can be recognized, for example, from the fact that out of the rest of sudden pain and tightness in the chest occur or the usual angina pectoris symptoms unusually difficult.
Call in case of unstable angina pectoris immediately the ambulance! The patient must go to the hospital as soon as possible because of the high risk of heart attacks.
Until the arrival of the emergency doctor you should First aid Perform: Loosen clothing that constricts the patient (e.g., collar, belt). Store his upper body and try to calm the patient. If it happens in a room, you can open the window and let in fresh air. This is what many sufferers find soothing.
Angina pectoris: drugs
An acute attack of angina pectoris is usually treated with nitro preparations such as nitroglycerin as a spray or capsule for biting. Nitro preparations expand the coronary vessels. This relieves the heart and lowers the oxygen consumption. Since the blood vessels in the rest of the body also expand, the blood pressure drops.
Nitro products should under no circumstances be taken together with sexual enhancers (phosphodiesterase 5 inhibitors) as they also lower the blood pressure. The blood pressure can then sink life-threatening deeply.
Other drugs that are used in angina therapy (including long-term), for example, drugs that keep the blood fluid (Antiplatelet such as acetylsalicylic acid or clopidogrel). Also called beta blocker Patients are often prescribed. They reduce heart rate and blood pressure under exercise. This can prevent angina pectoris attacks. Also helpful is the regular intake of vasodilators (Vasodilators) like different nitrates. Against elevated cholesterol levels, the doctor may call so-called statins prescribe.
Angina pectoris: heart surgery
The narrowed section of the vessel, which causes angina pectoris, can by means of balloon be stretched: A small plastic tube (catheter), a small balloon is introduced to the narrowed point in the vessel. On site, the balloon is inflated so that it expands the bottleneck.
Another way of treating angina pectoris is one Bypass surgery, The surgeon bridges the narrowed section of the vessel with a piece of the body’s own or artificial artery in order to restore the blood supply.
Angina pectoris: Healthy lifestyle
Patient involvement is also part of successful angina pectoris treatment: sufferers should adopt a lifestyle that avoids or at least reduces the risk factors of chest tightness. This succeeds, for example, with a healthy diet, regular exercise and abstinence from nicotine. Overweight patients should also try to lose weight. The attending physician can advise and assist patients in lifestyle change.
Angina: examinations and diagnosis
In case of suspected angina pectoris, the physician has various “tools” available to diagnose and hedge.
Conversation and physical examination
First the doctor talks to the patient To raise medical history (Anamnese). He asks, for example, when the symptoms of heart-beat have existed, how exactly they express themselves or whether they are triggered by anything (such as physical exertion). In addition, the doctor asks if the symptoms can be relieved with a nitrospray.
The information from the anamnesis interview will help the doctor assess whether the chest pain caused by a coronary heart disease (CHD) is another disease. For example, the symptoms can also come from the stomach. In addition, a pulmonary embolism (ie the occlusion of a pulmonary vessel by a blood clot washed ashore) can trigger similar symptoms to angina pectoris.
The next step is one physical examination at. Among other things, the doctor will listen to the heart and tap the breast. A blood pressure measurement is also part of this study. The doctor then checks if the patient has high blood pressure (hypertension).
Imaging procedures
Among other things, various imaging techniques help to test cardiac function and blood supply to the heart muscle:
Ultrasound of the heart: In cardiac ultrasound (echocardiography), the doctor uses ultrasound to examine whether the heart muscle has changed. So he can assess the heart chambers and heart valves and their function.
Rest and long-term ECG: An electrocardiogram (ECG) represents the electrical activity of all myocardial fibers as a sum in a cardiac tension curve. In more than half of patients with angina pectoris, the ECG is altered. If the doctor suspects cardiac arrhythmia, a long-term ECG is created.
Stress tests for the heart: Usually in the clinic or practice, a stress ECG is made with bicycle ergometry. The patient drives on a stationary bike while gradually increasing the load. At the same time the ECG and blood pressure values are measured. At a Exercise ECG The goal is to achieve inadequate blood flow to the heart muscle. If an angina pectoris occurs in the sequence and the ECG changes, one speaks of one positive ergometry.
Stress magnetic resonance imaging: Another possibility is the stress magnetic resonance imaging (stress MRI). The heart is medicated like drugs dobutamine and adenosine artificially charged (these agents make the heart beat faster and stronger). The doctor provokes a lack of oxygen in the heart and examines this or its consequences on MRI.
Herzszintigrafie: Cardiac or myocardial scintigraphy can represent the perfusion of the heart muscle. For this purpose, the patient first gets a weak radioactive substance injected. It is distributed according to the blood circulation in the heart muscle and is absorbed by the cells. The radioactive rays emitted by the substance are collected by a so-called gamma camera and displayed as a picture. The picture shows which areas of the heart muscle are less perfused. The pictures with the gamma camera are taken once at rest and once under load. Myocardial scintigraphy is used when ECG and echocardiography are not enough to diagnose angina pectoris.
Angina pectoris: course and prognosis
The chest tightness is usually an indication of atherosclerotic constricted coronary arteries (coronary heart disease, CHD) and therefore a warning signal. Arteriosclerosis develops slowly over years. At some degree, it can trigger angina pectoris even at low levels of stress. This can limit the quality of life and ability of the person concerned. The stronger and more common the attacks of angina pectoris, the higher the risk of heart attack.
It is therefore important to treat angina pectoris as early as possible. This not only means that the doctor prescribes the appropriate medication or performs an operation (balloon dilatation, bypass surgery). Every patient can positively influence the course of angina pectoris, for example by abstaining from smoking, a healthy diet and regular physical activity.
Angina: Prevention
If you want to prevent angina, the same tips apply in principle as for people who already suffer from chest tightness: A healthy lifestyle can make a major contribution to keeping the heart and blood vessels healthy. This is part of yourself to feed healthily, on regular physical exercise to pay attention and overweight to decrease, This reduces the risk of coronary heart disease (CHD), the most common cause of angina pectoris. Very important is also the Abstain from nicotineif you want to reduce your personal anginal risk. Because smoking narrows the vessels and thus affects the circulation of the heart muscle (and other body regions).
Also, go to regular checkups, Thus, diseases such as diabetes, high blood pressure or elevated blood cholesterol levels, which damage the vessels, can be recognized and treated in good time. If the doctor prescribes appropriate medication, you should take it regularly – even if you feel good at the moment.
Another tip: Avoid stress and treat yourself to regular rest in everyday life. This also helps one Angina pectoris submissions.
Additional information
guidelines:
- Guideline “Coronary heart disease / angina pectoris” of the German Society of Cardiology – Cardiovascular Research
Self-help:
- German Heart Foundation