In pulmonary emphysema, the alveoli are partially overstretched and destroyed. The result is that the body can no longer be sufficiently supplied with oxygen. Typical symptoms of emphysema include shortness of breath, shortness of breath and decreased performance. Smoking is the main cause of pulmonary hyperinflation. What other causes are there, what the consequences of pulmonary emphysema are and what the treatment and prognosis look like, read here!
Quick Tour
- What is pulmonary emphysema? Chronic lung disease associated with hyperinflation and destruction of alveoli. As a result, the body gets less and less oxygenated.
- Causes: Smoking, chronic inflammatory processes (chronic bronchitis, COPD etc.), alpha-1-antitrypsin deficiency, older age, inhalation of pollutants (dust, gases etc.), scarring in the lung tissue
- symptoms: Shortness of breath (first only with physical exertion, later also at rest), coughing, reduced efficiency, increased susceptibility to infection. In the advanced stage also blue lips and nails (cyanosis), barrel-shaped chest (Fassthorax), poor general condition with muscle loss, right heart failure (form of heart failure).
- investigations: Initial interview (anamnesis), physical examination, X-ray, computed tomography, blood gas analysis, pulmonary function test
- Treatment: Stop smoking, respiratory training, inhalation of saline, adequate fluid intake, drug therapy, in advanced emphysema, possibly long-term oxygen therapy, surgery. In very severe cases lung transplantation. Vaccinations against pneumococci and influenza viruses due to higher susceptibility to infections useful, treatment of acute respiratory infections with antibiotics.
- Forecast: No cure possible. Consistent treatment (especially smoking cessation) can slow down or stop the progression of the disease. Possible complications include pneumothorax (collapsed lung), right heart failure with water retention in the legs (edema), jammed neck veins, cirrhosis of the liver.
Pulmonary emphysema: knowledge & causes
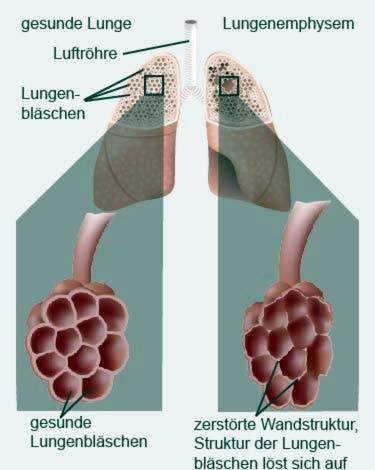
In pulmonary emphysema, more and more alveoli are pathologically over-inflated and destroyed. That’s why doctors also speak of one hyperinflation.
The alveoli are the smallest structural units of the lung and surrounded by a dense network of finest blood vessels (capillaries). Here, the gas exchange takes place: With every breath, air flows through the trachea into the alveoli. There, the oxygen from the air passes through the walls of the alveoli into the blood. At the same time carbon monoxide (CO2) is released from the blood to the air in the alveoli. This used air is then exhaled.
In pulmonary emphysema, the gas exchange is not working properly: For those affected The walls of the alveoli lose elasticity, Through the air flowing in with every breath the alveoli become overstretched, Finally, they can even burst, Neighboring destroyed alveoli then unite to bigger bubblesthat coincide when you exhale. Due to the hyperinflation of the alveoli, the smallest bronchi (bronchioles) are narrowed and also fall slightly together. Alltogether makes exhaling difficult: Patients can no longer exhale the inhaled air completely. Part of it remains in the remaining vesicles so that there is less room for new, oxygen-rich air during inhalation. An increasing Undersupply of oxygen is the result.
Pulmonary emphysema: causes
In the developmental mechanism of pulmonary emphysema, certain proteins usually play a decisive role:
With every inhalation, air and pathogens and other harmful substances enter the lungs. The immune system is usually armed against it: defense cells in the alveoli release regularly protein-degrading proteins, so-called proteases, They can destroy infiltrated germs and foreign substances. However, proteases do not distinguish between foreign and own tissue. They can therefore also attack and break down the sensitive lung tissue (more precisely, the elastic fibers in the walls of the alveoli). In order for this does not happen, usually a reasonable amount of protective proteins are released, the so-called Protease inhibitors, Their most important representative is Alpha-1 antitrypsin.
The balance between proteases and protease inhibitors may be due Smoke, chronic inflammatory processes as well as one Alpha-1 antitrypsin deficiency be disturbed so that increasingly lung tissue is broken down and pulmonary emphysema arises. Other possible causes are the repeated ones Inhalation of pollutants, higher age and scar tissue in the lungs.
Smoke
Smoking is the most common cause of emphysema. It inhibits protective protease inhibitors (such as alpha-1-antitrypsin). Thus, they can not prevent the attack of the proteases on the alveoli – pulmonary emphysema develops.
Chronic inflammatory processes
Chronic inflammatory processes in the lungs, like smoking, can cause the destructive proteases in the alveoli to gain the upper hand. In this way, both chronic bronchitis and chronic obstructive pulmonary disease (COPD) can pave the way for pulmonary emphysema.
Alpha-1 antitrypsin deficiency
About one percent of patients develop emphysema based on a genetic deficiency of alpha-1-antitrypsin, the major protease inhibitor. The affected are thus more susceptible to pulmonary emphysema than the normal population. The level of disease risk in each individual case depends on the severity of the hereditary disease. Pulmonary emphysema develops particularly easily when people with congenital alpha-1 antitrypsin deficiency additionally smoke or have chronic lung disease (such as COPD).
A congenital alpha-1-antitrypsin deficiency can have further consequences in addition to pulmonary emphysema. This includes an increasing destruction of liver cells (liver cirrhosis).
Age
With age, the elasticity of connective tissue generally decreases. This also reduces the elasticity of the partitions of the alveoli. This rarely leads to the development of age-related pulmonary emphysema. This so-called Altersemphysem is not a disease, but a consequence of the natural aging process. The affected people usually show no symptoms. Therefore, the age emphysema usually does not need to be treated.
scar tissue
After a lung infection or tuberculosis and after a lung operation (such as removal of a lung), scar tissue often develops in the lungs. This is more unstable than normal lung tissue and is therefore more easily overstretched. This creates a so-called Narbenemphysem.
Respiratory tract irritants
Rarely, pulmonary emphysema develops through inhalation of irritating gases or dust. These inhaled noxae include:
- quartz-containing dust
- Cotton and cereal dust
- welding fumes
- Gases such as ozone or chlorine gas
The general air pollution in large cities can also promote emphysema. This is especially true for people who already have another lung disease.
Types of emphysema
There are different types of emphysema. In the classification, the cause of lung overstretching plays an important role:
- Centrilobular emphysemaAbout one-third of chronic pulmonary emphysema patients suffer from a centrilobular form. In particular, the upper lung fields are affected, while the lower ones are intact. Physicians attribute this to the fact that pollutants such as cigarette smoke first reach and damage the upper lung tissue.
- Panlobular pulmonary emphysema: This type of pulmonary emphysema is mostly genetic, so it is based on the congenital alpha-1-antitrypsin deficiency described above. Here, especially the alveoli of the lower lung sections are affected.
- Overexpansion emphysemaIf some part of the lungs have to be surgically removed, the residual lung sometimes overstretches – causing over-emphysema. Compared to the two other types of emphysema, it usually causes less discomfort, as the walls of the alveoli have not previously been damaged by chronic inflammation (caused, for example, by cigarette smoke).
Pulmonary emphysema: symptoms
Pulmonary emphysema symptoms develop slowly and slowly. The type and severity of the symptoms depend on the stage of the disease.
First emphysema symptoms
In the initial stage pulmonary emphysema patients are usually under Shortness of breath during physical exertion, Add to that sporadic cough and areduced efficiency. Many sufferers get tired easily even with a light effort.
Also frequent infections of the respiratory tract such as bronchitis and pneumonia are typical accompanying symptoms of pulmonary emphysema. This susceptibility to infection results from the increasing destruction of the ciliated epithelium, which lines a large part of the respiratory tract. The cilia are similar to small hairs. They move undulating and transport tiny foreign particles out of the lungs (mucociliary clearance). However, tobacco smoke and other pollutants destroy the ciliated epithelium long term, which disturbs the cleaning mechanism. That facilitates infections.
Advanced pulmonary emphysema
Show people with advanced emphysema Respiratory distress already in peaceSo without physical effort. In addition, many patients suffer Cough with slimy expectoration, especially if there is chronic bronchitis at the same time.
Increasing pulmonary hyperinflation can alter the shape of the ribcage over time. In pulmonary emphysema, the chest muscles are more stressed during breathing and remain permanently in the inhalation position. The ribs then run horizontally instead of sloping downwards, and the rib cage appears “barrel-shaped” (Barrel thorax), The two skin pits above the clavicles disappear – they are also over-inflated in many people affected.
Frequently, the general condition of the patients also deteriorates. As a result of shortness of breath, those affected move less, leaving the body Loss of muscle, This can further increase dyspnea.
The persistent lack of oxygen in the blood is often seen through blue discolored lips and fingers (cyanosis), In addition, the over-inflated lungs can overload the right side of the heart. This is how a particular form of heart failure (heart failure) develops: the right heart failure, The overloaded right half of the heart can not transport the inflowing blood sufficiently. It backs up into the systemic circulation. This congestion shows up among other things bulging neck veins, Further signs of right heart failure are Water retention in the legs (edema).
Two extremes: Pink Puffer and Blue Bloater
Pulmonary emphysema patients are divided into two types: the “Pink Puffer” and the “Blue Bloater”. Both are extreme forms that are rarely observed in their full extent. Mostly the transitions are fluent.
Typical features of the Blue Bloater are:
- overweight
- pronounced cyanosis (blue coloration of the lips and fingers, hence the term “Blue Bloater”)
- severe cough with sputum
- barrel chest
- slight breathlessness
- “Lips brake” (exhale through loose lips)
Typical features for the Pink buffer are:
- underweight
- no cyanosis due to heavy work of breathing, rather pale skin color
- pronounced respiratory distress
- dry cough without expectoration
Expressed in a simple way: The “Pink Puffer” fights against his pronounced respiratory distress, breathing consciously and intensely. As a result, his blood is sufficiently saturated with oxygen, so that no cyanosis arises. In contrast, the “Blue Bloater” gets used to the chronic oxygen shortage over time, which often leads to right heart failure due to a so-called cor pulmonale. At the same time, the right heart is depleted, as it has to pump against too much resistance in the pulmonary circulation.
Pulmonary emphysema: treatment
Pulmonary emphysema is not curable. This means that the pathological changes in the lung tissue are irreversible (irreversible). With the right therapy, however, the course of the disease can be slowed or even stopped.
Do not smoke!
Patients with pulmonary emphysema should immediately and permanently stop smoking. Some people stop smoking altogether. But many need help. After all, nicotine addiction is considered one of the strongest dependencies. So do not hesitate to seek help with smoking cessation. This can be a behavioral therapy or a self-help group. Also, nicotine substitutes such as nicotine patches, gums or sprays as well as acupuncture or hypnosis can help with weaning.
Vaccinate
Pulmonary emphysema patients are more prone to respiratory infections. Therefore, doctors recommend the pneumococcal vaccine and the flu vaccine. The vaccine protection of the pneumococcal vaccine lasts for about five years and should then be renewed. You need to be vaccinated every year against flu (influenza), as influenza viruses are constantly changing.
Treat infections early
Fever and cough with yellow-greenish expectoration indicate a bacterial respiratory tract infection. If pulmonary emphysema patients show such symptoms, they should be treated by the doctor with antibiotics. This can prevent a serious illness. Rarely, a long-term antibiotic treatment is necessary, which the family doctor then has to closely monitor.
Medical therapy
Which drugs are used in pulmonary emphysema depends on the stage of the disease and the severity of the symptoms. In principle, the following active ingredients are available (in principle the same as in the treatment of asthma and COPD):
- Beta2-adrenergic agonist: act as bronchodilators and are inhaled; there are short-acting (such as salbutamol, reproterol) and long-acting representatives (such as salmeterol)
- anticholinergics: they also act as bronchodilators and are inhaled; Example: Ipratropium
- if necessary glucocorticoids (“cortisone”): anti-inflammatory effect; are also usually inhaled; only in severe cases you may give cortisone tablets
In the case of a congenital alpha-1 antitrypsin deficiency, the missing protein can also be replaced by medication. Such Alpha-1 antitrypsin substitutes are given regularly as an infusion.
Long-term oxygen therapy
Patients with severe emphysema often receive long-term treatment with oxygen: pure oxygen is inhaled through a mask for at least 16 hours daily. This can improve the prognosis and increase the quality of life of those affected.
But not all patients benefit from an oxygen therapy. Has the body already at an elevated C02Used to levels in the blood, eliminates the strongest breath drive: just the rising C02-Salary. Then the lack of oxygen remains as the only respiratory drive. If now uncontrolled oxygen supplied, also eliminates this last respiratory drive. Patients stop breathing autonomously and may develop carbon monoxide narcosis. Therefore, the doctor decides very carefully whether an oxygen therapy in pulmonary emphysema in individual cases makes sense or not.
During an oxygen therapy, you should not smoke, because oxygen is highly explosive. Just a little embers or a small spark is enough to ignite the gas!
Physical pulmonary emphysema therapy
At a respiratory therapy The patients learn special techniques that make exhaling easier. Helpful for the right breathing technique are also strong abdominal muscles. Therefore, the therapy also includes targeted abdominal training, In addition, sufferers should drink adequately and inhale regularly with saline solution to aid in coughing up the sputum.
surgery
For severe pulmonary emphysema, surgery may be useful. The doctor removes the functionless, over-inflated lung tissue (Volume reduction therapy). As a result, the healthy lung tissue is better ventilated again.
In patients with very advanced pulmonary emphysema, the last treatment option often remains one lung transplantation.
Pulmonary emphysema: examinations and diagnosis
The right contact for suspected emphysema is a Specialist in pulmonology (pneumologist), He will talk to you in detail first about yours medical history to raise (anamnesis). Possible questions during this conversation are:
- Do you suffer from shortness of breath?
- Do you often cough? Is the cough dry or associated with ejection?
- Do you have any other complaints?
- Do you smoke? If so, how much and how long?
- How many stairs can you climb without having to take a break?
- Do you already have lung disease (asthma, chronic bronchitis, etc.)?
- Do you have relatives who suffer from emphysema, COPD or alpha-1-antitrypsin deficiency?
Physical examination
The medical history is followed by a physical examination. The doctor can detect typical changes that may indicate pulmonary emphysema. This includes about the so-called barrel chest: A barrel-shaped altered thorax speaks for a permanent lung hyperinflation. This is a clear hallmark of pulmonary emphysema.
Characteristic is also the instinctively executed pursed lip during exhalation. In the process, the affected persons breathe out through the loosely laid-up lips. This breathing technique makes exhaling easier, because it increases the air pressure in the bronchi.
Bluish discolored lips and fingers are also serious signs of pulmonary emphysema. The same applies to the so-called Drumstick fingers and watch glass nails, The fingers are distended on the end members like drumsticks, while the fingernails are strongly rounded.
Important signs are also swollen legs and bulging neck veins, They indicate that the right half of the heart is under increased strain. The reason for this can be emphysema.
When listening to the lungs with the stethoscope (auscultation) are often in pulmonary emphysema dry rattle sounds to hear (a humming or whistling). When tapping the ribcage (percussion) it sounds loud and hollow, The reason is the increased amount of air in the over-inflated lung. In contrast, the Heart sounds often very quiet to hear with the stethoscope due to the volume enlargement of the lungs.
Further investigations
To assess how far emphysema is already advanced, the doctor can check the rib cage roentgen (X-ray thorax): The excess air trapped in the alveoli may force the diaphragm down (flatten) and appear as a dark area on the x-ray. In addition, the usually highly visible vessels are often poorly recognized (vascular rarification).
With a Computed tomography (CT) the emphysema of the lung can be shown in more detail.
Whether an emphysema patient is Pink Puffer or Blue Bloater, the doctor can use one Blood gas analysis and one Pulmonary function tests detect. These diagnostic methods show if only the oxygen content in the blood is reduced (typical for the Pink Buffer) or whether the CO2Level is elevated (typical of the Blue Roater).
Pulmonary emphysema: disease course and prognosis
Cure emphysema is not curable. However, if one adheres to the treatment plan prescribed by the doctor, one can slow down or even stop the disease process.
One of the most important therapy building blocks is the immediate, absolute and permanent smoking cessation!
Pulmonary emphysema: complications
Consistent therapy is also important given the complications that progressive emphysema can bring: pneumothorax and right heart failure.
pneumothorax
A serious acute complication of pulmonary emphysema is pneumothorax: there is usually a negative pressure in the cleft between the lung and the pleura (pleural space). However, if an emphysema-damaged alveoli bursts, air can penetrate into the gap and release the negative pressure – with grave consequences: The lung collapses on the affected side. The collapsed part is no longer ventilated and can therefore no longer participate in the gas exchange. A spontaneous pneumothorax usually goes through one sudden, stabbing pain and shortness of breath noticeable.
Right heart failure
Pulmonary emphysema increases the pressure in the pulmonary vessels over time. The right half of the heart has to inflate against the increased resistance in the pulmonary vessels, which puts increasing strain on them. Over time, this can lead to right heart failure (right heart failure). The weakened right half of the heart (cor pulmonale) can not pump enough, so that fluid in the legs (edema) collects. In addition, it can lead to cirrhosis and congested neck veins.
To avoid these complications, you should strictly adhere to the treatment guidelines of your doctor and above all stop smoking. Then there are good chances, that emphysema unstoppable.
Additional information
Support Groups:
- Patient organization pulmonary emphysema-COPD Germany
- COPD Germany e.V.