In a pleurisy (pleurisy), the ribs and usually also the lung in the chest inflamed. These are the connective tissue envelopes around the lungs and on the inner wall of the rib cage. Typical symptoms include aches and pains when breathing “dry” pleurisy. When fluid accumulates, it is called “wet” pleurisy. Read all important information about signs, causes and therapy pleurisy!
Quick Overview
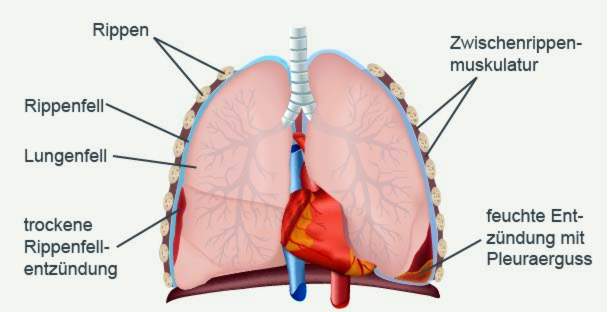
- Definition: In pleurisy (also pleurisy, pleurisy), the pleura, the pleura, inflamed. This two-part layer of tissue coats the chest cavity (pleura) and covers the lungs (lung pelt).
- Watch out: Even though one usually speaks of pleurisy, the second layer of the pleura, the lung pelt, is usually also inflamed.
- symptoms: severe, breath-dependent pain when breathing (“dry” pleurisy); in “wet” pleuritis, decreasing pain and, if necessary, difficulty in breathing, including respiratory distress with large accumulation of fluid (pleural effusion); possibly fever
- Causes: Pneumonia, pulmonary embolism, pulmonary infarction, tuberculosis, viral infection (coxsackie B virus), autoimmune diseases (such as lupus erythematosus, rheumatoid arthritis), cancers etc.
- Treatment: Treatment of the underlying disease (e.g., antibiotics for bacterial infection). Otherwise relief of symptoms, for example, with analgesics and antipyretic drugs.
Pleurisy: symptoms
A pleurisy (or pleurisy) may cause different symptoms – depending on whether it is a “dry” pleurisy or one “wet” pleurisy is. The difference between the two is found in the so-called Pleural space (pleural cavity): This is the narrow, slightly fluid-filled space that separates the two thin leaves of the pleura:
The inner tissue layer of the pleura is called the lung pelt and covers the lungs. Externally, the pleura joins, lining the chest cavity inside. The ribs and pleura are connected to each other at an umber fold at the edge of the lung.
The fluid between the lung and the pleura, ie in the pleural space, can change during pleurisy:
- “Dry” pleurisy (Pleuritis sicca): no additional fluid in the pleural space. In most cases, however, threads of fibrin (coagulation protein) are formed here, which intensifies the friction between the two leaves of the pleura.
- “wet” pleurisy (Pleurisy exudative): additional accumulation of fluid between lung and pleura (pleural effusion)
Often a pleurisy affects only one side of the body. The left and right lungs, together with the pleural cavities, are separated from each other by the middle medullary space (mediastinum).
“Dry” pleurisy: symptoms
When a pleurisy usually both the pleura and the lung are inflamed. Only the pleura is sensitive to pain – but all the more so. The friction created by breathing between the two skins causes dry pleurisy severe, breath-dependent and stabbing chest pain, The deeper the patient inhales, the more it hurts. That’s why many patients only breathe flat. Some also instinctively adopt a posture that relieves the inflamed side.
The dry pleurisy can also be painful to cough be accompanied. The pain usually occurs on one side. Depending on the severity of the inflammation, it can radiate to the shoulder.
Also typical for a pleurisy is a creaking or rubbing breath sound, the so-called leather rubbing. It arises because the pleura and pleura rub together in the inflamed areas with each movement of the ribcage.
If the pleurisy attacks the diaphragm (the muscle plate that lies under the lungs), hiccups can also occur.
“Damp” pleurisy: symptoms
With a pleural effusion, more fluid accumulates in the pleural space than normally. This can generally have different causes. If the pleural effusion forms in the course of a pleurisy, physicians speak of “Pleurisy exudativeSymptoms such as pain and rubbing of the leather are either absent or greatly reduced, and the effusion between the inflamed pleura leaves prevents them from rubbing against each other.
This often shows other symptoms in this form of rhinitis: Signs of pleural effusion may be a difficult breathing or even difficulty in breathing (Dyspnea). This happens when the effusion is so great that it squeezes the lung significantly. With a small effusion the patient can breathe normally.
Transition from dry to damp
Often a moist pleurisy develops from a dry one. This means that the inflammation causes fluid to escape from the fine blood vessels (capillaries) and collects as an aqueous effusion in the pleural space. If the Pleural effusion purulent is, doctors speak of one pleural empyema, But he can also mostly blood consist (hemorrhagic pleurisy).
Sometimes accompanied fever the transition from a dry to a “wet” pleurisy.
Previous illness influences symptoms
Other symptoms of pleurisy depend on the underlying disease. Some examples:
At a lung infection High fever with chills and cough with sputum often occur. The pleurisy develops as a result of tuberculosisMany patients also suffer from coughing, fatigue and night sweats.
At a Coxsackie B virus infection (Bornholm disease), sufferers have difficulty breathing as well as spasmodic pain in the chest and upper abdomen. Such pains can also occur if pleurisy is the result of upper abdominal disease, for example, one pancreatitis (Pancreatitis).
Also cancers such as a malignant tumor of the pleura (pleural mesothelioma) are possible causes of pleurisy. Signs of pleural mesothelioma are more advanced than those of “normal” pleurisy.
Pleurisy: causes
A pleurisy can have various causes. Mostly it occurs concomitant or as a result of another disease on, for example:
- Pneumonia
- tuberculosis
- Coxsackie B virus infection (Bornholm disease)
- Tumors in the area of the pleura
- Connective tissue diseases (collagenosis) such as lupus erythematosus or rheumatoid arthritis
- Pulmonary embolism, pulmonary infarction
- Urea poisoning (uremia)
- Upper abdominal diseases such as pancreatitis
The most common underlying disease of pleurisy is one lung infectionThe inflammatory processes can relatively easily spread from the lungs to the pleura.
The pleura can also be damaged directly, such as through Coxsackie B viruses or as a result of Illnesses in the upper abdomen (like pancreatitis). Also the tuberculosis comes as a trigger of pleurisy in question. However, this so-called “pleuritis tuberculosa” has become rare in Central Europe.
A pleurisy with a bloody pleural effusion may be indicative of a so-called pleural be. The term used by medical professionals, when a malignant tumor has formed secondary tumors (metastases) in the area of the pleura. This can happen, for example, in lung cancer and breast cancer.
In rare cases, the cells of the pleura develop into cancer cells themselves. This is how you get started primary tumor of the pleura (Pleural). This can trigger pleurisy. Incidentally, a pleural mesothelioma mainly affects people who have come into contact with the construction and industrial fabric asbestos.
Pleurisy: examinations and diagnosis
First, the doctor conducts a detailed conversation with the patient to whom To raise medical history (anamnesis), He can describe the occurring complaints exactly. In addition, the doctor asks if other illnesses (past or present) are known, such as pneumonia, tuberculosis or a tumor. If so, the doctor will ask what therapies and medical procedures have been performed.
Physical examination
After the anamnesis interview follows one physical examination, Sometimes the doctor may already be at the posture of the sufferer recognize that something is wrong with breathing on one side of the lungs. In addition, the body side, where the pleurisy is located, usually less involved in the respiratory movements. This is called “Dragging” designated.
More detailed instructions provide that Tapping and listening to the ribcage, Typically, in a pleurisy with the stethoscope can hear a creaking breath sound, the so-called leather rubbing. However, in pleural effusion with pleural effusion (pleurisy exudative), the sound is only attenuated or not heard at all.
Also from the Knocking sound the doctor can gain valuable information. A muted knocking sound can, for example, indicate a fluid accumulation (pleural effusion).
Imaging procedures
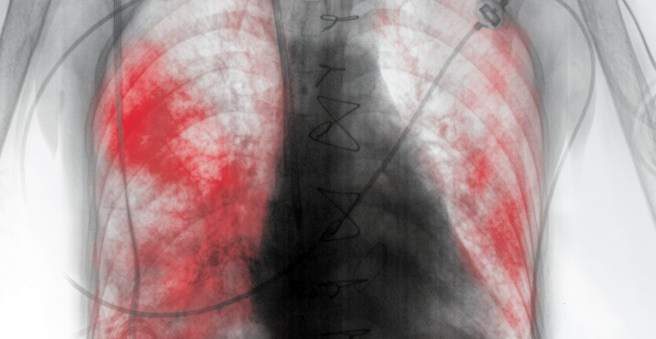
For the diagnosis of pleurisy is a X-ray of the ribcage (chest x-ray) is particularly important. In most cases, the doctor makes shots of the chest from the front and from the side. A “dry” pleurisy is inconspicuous on the radiograph. In contrast, a pleural effusion is usually easy to recognize.
To make small or difficult to detect fluid collections visible, the doctor can ultrasound and optionally also one Computed tomography (CT) carry out.
The various imaging techniques not only help with the diagnosis of “pleurisy”. Often they also serve to clarify the cause of the inflammation. For example, imaging can visualize tuberculosis or tumors.
Further investigations
A blood test is also important in pleurisy. Using various inflammatory parameters (such as blood cell count, CRP, white blood cells, etc.), the doctor can estimate how pronounced the inflammatory processes are.
If the doctor suspects that pleurisy is caused by an autoimmune disease (such as lupus erythematosus), this can also be clarified for a blood test. It is checked whether antibodies can be detected in the patient’s blood, which falsely attack the body’s own tissue (such as the pleura) (autoantibodies).
When looking for the cause of pleurisy it can also help the Analyze the fluid in the pleural space, To do this, the doctor pricks between the ribs with a thin hollow needle and pushes it to the pleural effusion to take a small sample (pleural function). The liquid is then carefully examined in the laboratory, for example for the presence of blood, pathogens (such as tuberculosis bacteria) or tumor cells.
In some cases, one is also Reflection of the ribcage (Thoracoscopy) makes sense. The doctor makes a small opening in the chest wall and inserts a laparoscope over it. It is equipped among other things with a small camera and a light source. This allows the doctor to examine the pleural cavity from the inside.
Pleurisy: treatment
For every treatment of pleurisy it belongs, the To treat underlying disease.
For example, when bacteria are the trigger (as in tuberculosis or bacterial pneumonia), the patient receives antibiotics, These fight the pathogens directly. In addition, the symptoms are treated as needed, for example with painkillers and antipyretic drugs.
In other cases, viruses (e.g., Coxsackie B viruses) are the causative agent of pleurisy. The treatment is limited here to alleviate the symptoms of the patient (painkillers, antipyretics, etc.). Drugs that help specifically against the viruses (such as antibiotics against bacteria) are not available here.
With a “damp” pleurisy, it may also be necessary, the pleural effusion to remove specifically. The doctor usually leads a so-called chest tube through: A thin tube is advanced into the pleural space via a small opening in the chest wall. Then the effusion is sucked off. If necessary, the pleural cavity can also be rinsed with saline and antibiotics.
For example, chest drainage is necessary if the pleural effusion is quite large and causes respiratory distress. Even with a purulent effusion, the procedure is performed. By contrast, the body can usually eliminate smaller, watery effusions by itself.
Pleurisy: disease course and prognosis
The course of the disease depends on the cause and the severity of pleurisy. Duration and prognosis can vary widely, depending on how quickly and successfully pleurisy can be treated. But especially in young people, pleurisy usually has a good prognosis.
If the inflammation persists for an extended period of time, the pleura and pleura can grow scarred together. Large adhesions after one pleurisy It is also referred to as Pleuraschwielen or Pleuraschwarten. In extreme cases, these calluses may also calcify (pleurisy calcarea). This restricts breathing permanently.