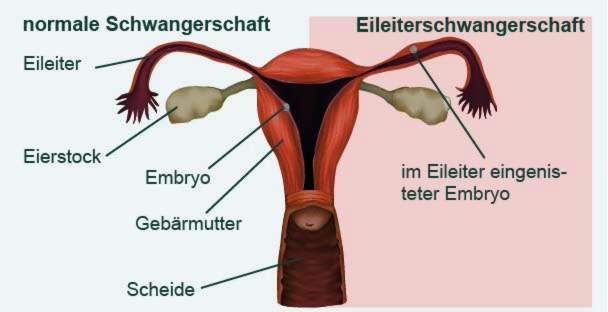
In an ectopic pregnancy, the fertilized egg does not nest in the uterus, but in the fallopian tube. This can happen if the fallopian tube is not completely permeable. Due to the growing embryo, the fallopian tube can break. Life-threatening bleeding in the abdominal cavity is the result. Since the symptoms of an ectopic pregnancy are hardly different from those of a normal pregnancy, only a specialist can make the diagnosis. Read more about ectopic pregnancy here!

Quick Overview
- What is an ectopic pregnancy? Pregnancy, in which the fertilized egg is implanted in the fallopian tube instead of the uterus. Most common form of extrauterine pregnancy (pregnancy with implantation of the embryo outside the uterus).
- Causes: Not or not completely permeable fallopian tubes. Various risk factors, such as glued or bent fallopian tubes, ectopic polyps, previous infections of the tubes, previous ectopic pregnancies, abdominal or pelvic operations, smoking, spiral, fertility disorders, artificial insemination, etc.
- symptoms: Labor-like abdominal pain, vaginal bleeding, dizziness, circulatory problems, general malaise.
- Complication: Fallopian tube rupture with severe bleeding into the abdominal cavity and circulatory shock (mortal danger!).
- Treatment: Depending on the stage of ectopic pregnancy. Mostly surgical removal of the embryo, if possible with preservation of the affected fallopian tube. At a very early stage possibly drug treatment. Sometimes waiting under medical supervision (the Embyro can spontaneously go off alone).
- Forecast: With proper treatment, complete healing. Later pregnancies can be quite normal.
Ectopic pregnancy: description and causes
Ectopic pregnancy (tubal pregnancy) is the most common form of so-called ectopic pregnancy (around 96%).ectopic pregnancy, EUG). These are pregnancies in which the fertilized egg cell is implanted outside the uterus (ectopic implantation). In the case of ectopic pregnancy, the ovum is stuck in the fallopian tube. In other forms of extrauterine pregnancy, the ovum nests in the ovaries (ovarian pregnancy), the cervix (cervical pregnancy) or in the abdominal cavity (peritoneal pregnancy). It can not be discharged.
Extrauterine pregnancy accounts for one to two percent of all pregnancies.
Forms of ectopic pregnancy
Depending on where in the oviduct the ovum is implanted, physicians distinguish three forms of tubal pregnancy:
- Ampullary ectopic pregnancy: The implantation takes place in the first third of the fallopian tube.
- Isthmic ectopic pregnancy: The fertilized egg cell nests in the last third of the fallopian tube, just before it flows into the uterus.
- Interstitial / intramural pregnancy: The fertilized egg cell nests at the transition from the fallopian tube to the uterus.
An ectopic pregnancy can not be carried out. Without treatment, the growing embryo can rupture the fallopian tube. This causes a life-threatening bleeding in the abdominal cavity.
Causes of an ectopic pregnancy
Normally, the fertilized egg migrates through the fallopian tube into the uterus and nests there. But if the fallopian tube is not permeable or only partially permeable, the egg remains stuck in it on its way into the uterus and grows firmly. The patency of a fallopian tube may be affected for various reasons. These include:
- Gluing or kinking of the fallopian tube
- tubal polyps
- Inborn anatomical features such as cavities in the fallopian tube wall
- Scarring or adhesions of the euthanist, for example due to previous operations in the abdominal or pelvic area
- Ear infections, especially those caused by chlamydia.
- earlier ectopic pregnancies
- Fertility disorders and artificial insemination
- local damage to the fallopian tubes, such as endometriosis (foci of dislocated uterine lining, for example, in the fallopian tubes)
- abortions
- miscarriages
- muscle weakness
- Too little cilia on the inner wall of the fallopian tubes (the hair-fine cilia drive the egg in the fallopian tube)
- Taking the “morning after pill”
- hormonal imbalance
- tuberculosis
It also favors Smoke the emergence of an ectopic pregnancy. Nicotine restricts the mobility of the cilia.
Also, women with one spiral prevent, have an increased risk: The spiral facilitates microorganisms access to the fallopian tubes, where they can cause inflammation. These in turn favor an ectopic pregnancy.
The number of ectopic pregnancies has increased in recent decades. Experts discuss various causes, including increased tubal inflammation as a result of sexually transmitted diseases, more frequent fertility treatments, the use of spirals as a contraceptive, and smoking.
Ectopic pregnancy: recognize symptoms
An ectopic pregnancy initially runs like a normal pregnancy:
- Absence of the period
- Nausea in the morning (possibly at other times of the day)
- Tension in the breasts
Even one pregnancy test can not distinguish between a normal and an ectopic pregnancy. He also indicates a positive result with the latter. Because the placenta (mother cake) forms the pregnancy hormone beta-HCG (Human Chorionic Gonadotropin) in an ectopic pregnancy as in a normal pregnancy, to which the test reacts positively.
Ectopic pregnancy: signs
The signs of ectopic pregnancy typically show up first between the sixth and ninth week of pregnancy, They include:
- unusual, usually one-sided, convulsive or labor-like pains in the abdomen
- Tense abdominal wall, which reacts sensitively to touch
- Vaginal bleeding (often as a slight brownish discharge = spotting, sometimes dark red with clots of clotted blood and / or tissue)
- Dizziness and paleness
- difficulty in breathing
- raging pulse
- Nausea and vomiting
- general malaise
- slightly elevated temperature
The symptoms of an ectopic pregnancy can be different from woman to woman be. They can also be sudden and intense, or slowly increase.
The symptoms mentioned are not specific to ectopic pregnancy. Similar symptoms can also occur with kidney inflammation, appendicitis, ovarian inflammation or tubal inflammation. Only a doctor can determine the exact cause of the symptoms.
Ectopic pregnancy: complications
In about three out of ten women with ectopic pregnancy complications occur: Through the growing embryo ruptures the fallopian tube. Important blood vessels (usually the uterine artery or the arteria ovarica) are injured. The consequences are severe internal bleeding. Warning signs are sudden onset, very strong, one-sided pelvic pain that can radiate to the upper abdomen, back and shoulder. Blood loss can cause dizziness, fainting or a circulatory shock.
If there is evidence of ectopic pregnancy you should seek medical attention immediately. If it comes to the Eileiterriss there is danger to life! Then alert the ambulance immediately!
Ectopic pregnancy
A very rare abdominal cavity pregnancy is like ectopic pregnancy a form of extrauterine pregnancy: The fertilized egg cell falls through the upper opening of the fallopian tube into the abdominal cavity and nests here – usually on the intestinal wall or the back wall of the uterus.
In most cases, an abdominal cavity pregnancy is discovered as part of screening ultrasound examinations. The embryo in the abdominal cavity is usually not viable. In most cases, he dies off by himself. If that does not happen, it will be surgically removed.
You can find out more about this topic in the article “Intestinal Pregnancy”.
Ectopic pregnancy: examinations and diagnosis
The Gynecologist (gynecologist) is at first suspected of having an ectopic pregnancy in conversation with the patient To raise medical history (Anamnesis): He gives a detailed description of the symptoms and inquires about possible risk factors (previous ectopic pregnancies, oviditis, miscarriages or abdominal surgery, endometriosis, etc.).
Gynecological check
After that follows one vaginal palpation: Internal and external palpation is part of the normal gynecological examination. The doctor can gain important information from this. If there is an ectopic pregnancy, the uterus is smaller than it should actually be due to the current week of pregnancy. The physician may also notice during palpation that a fallopian tube is enlarged on one side.
The palpation of the fallopian tube in which the embryo has lodged may cause some pain.
Ultrasonic
Where exactly a fertilized egg cell has established, can usually be by means of a ultrasound determine. It can be done via the vagina (transvaginal sonography). This indicates whether a normal pregnancy is present (ie with implantation in the uterine cavity). If there is no oocyte in the uterus, it may be for the following reasons:
- The embryo has settled in the womb, but is still too small to be detected by ultrasound. The pregnancy is then less advanced than one had assumed on the basis of the last menstrual period observed.
- Although the embryo was in the uterus, it was rejected (miscarriage, abortion).
- The embryo has actually established itself outside the uterus (extrauterine pregnancy such as ectopic pregnancy).
To examine the third option, the gynecologist can apply a special variant of the ultrasound examination, the Farbdopplersonografie, It is particularly good at visualizing perfused tissue – for example, the area of the mucous membrane in which the egg has taken root (in the fallopian tube, for example).
blood test
In addition, the doctor can determine the amount of pregnancy hormone Beta-HCG (Human Chorionic Gonadotropin) in the blood of the pregnant woman several times over a long period of time. In normal pregnancies, the blood level of this hormone doubles every two days. In contrast, if the egg cell has lodged incorrectly (as in an ectopic pregnancy), the HCG level rises only slowly, stagnating or even sinking again.
laparoscopy
In unclear cases, the doctor may additionally laparoscopy (Laparoscopy). It can be determined with certainty whether an ectopic pregnancy actually exists. If so, the malignant ovum can be removed immediately during the examination (see: treatment).
Ectopic pregnancy: treatment
Depending on how far the ectopic pregnancy has progressed, different treatment approaches result.
laparoscopy
If an ectopic pregnancy is associated with abdominal pain, incipient bleeding in the abdominal cavity, or abnormal HCG level, usually one must laparoscopy (Laparoscopy). This allows the extrauterine pregnancy to be recognized and treated at the same time. During the procedure, the doctor introduces a so-called endoscope into the abdominal cavity via three small incisions in the abdominal wall. This is a thin, flexible tube with a light source and a small camera on top. The doctor can use the endoscope to introduce the finest medical instruments to remove the embryo from the fallopian tube.
Open operation
In some cases of ectopic pregnancy is an open surgery (laparotomy): The surgeon opens the abdominal wall with a larger incision to remove the embryo in the fallopian tube. An open surgery is necessary, for example, if a laparoscopy is not possible for certain reasons, the woman has extensive adhesions or an unstable circulation. Even in cases in which the ectopic pregnancy has already led to a fallopian tube, must be operated on open. This is the only way to stop the heavy bleeding as quickly as possible.
If the bleeding is very severe or the fallopian tube is severely damaged, it sometimes has to be completely removed. The doctors, however, always try to get the fallopian tube if it is possible.
drugs
A very early ectopic pregnancy can also be treated with medication in individual cases. The pregnant woman is usually administered the drug methotrexate. The doctor injects the cell poison under ultrasound control into the amniotic sac, causing the embryo to die. In the days thereafter, the doctor regularly checks whether the level of beta-HCG in the blood of the pregnant woman is falling. This decrease indicates that the pregnancy has actually ended.
The drug treatment is possible only under certain conditions. Thus, the ectopic pregnancy must not cause any discomfort. In addition, the embryo, together with the surrounding tissue, must be smaller than four centimeters. Last but not least, the level of HCG in the blood of pregnant women must be below a certain threshold.
Wait and watch
Many ectopic pregnancies terminate by themselves within the first three months of pregnancy. Since the fallopian tube does not provide sufficient space for the growing embryo and can not ensure its adequate supply, the oocyte bursts. Platzenta and fruit sack then separate from the fallopian tube wall. They go naturally with the embryo.
So if no symptoms and at the same time the level of the pregnancy hormone beta HCG in the blood is exceptionally low, you can possibly with a therapy wait a few days, The pregnant woman is carefully monitored. If the concentration of the pregnancy hormone continues to decrease during this time and the embryo no longer grows, the pregnancy is likely to be over. However, if the embryo continues to grow, the fallopian tube can break within a very short time and lead to a dangerous bleeding. One must be prepared for this possibility: It must be ensured that in such an emergency, the pregnant woman can be operated on quickly.
Ectopic pregnancy: history and prognosis
Often, an ectopic pregnancy goes unnoticed and ends by itself – the wrong eingiistete egg cell is repelled along with the placenta. If this does not happen, the ectopic pregnancy should be stopped as soon as possible with surgery or medication.
The drug treatment is considered to be more gentle for the affected fallopian tube than surgery, but is only possible in certain cases. If a surgical procedure (laparoscopy, open surgery) can not be avoided, the fallopian tube can be preserved in most cases. Its patency is usually 80 to 90 percent after surgery. Incidentally, the same applies if the ectopic pregnancy is treated with medication.
different factors. For example, it affects how much the fallopian tube has been damaged by the ectopic pregnancy, whether it needs to be removed, and how well the second fallopian tube works. It also has an influence whether the woman already had more than one extrauterine pregnancy. For example:
After a first ectopic pregnancy, which was terminated surgically (with the affected fallopian tube being preserved), the risk of a second such ectopic pregnancy is about 15 percent. Had a woman already two tubal pregnancies, the “repetition risk” is about 40 percent.
In general, however, more than half of all women, the one ectopic pregnancy (or other extrauterine pregnancy), later still have a child.