The heart muscle inflammation (myocarditis) is a serious illness. It often develops as a result of influenza infections. Their symptoms are often difficult to detect, which makes a quick diagnosis difficult. In severe cases, myocarditis may cause heart failure or severe cardiac arrhythmias. Then there is even a risk of sudden cardiac death. Read here how you can recognize myocarditis, how it develops and how to treat it.

Quick Overview
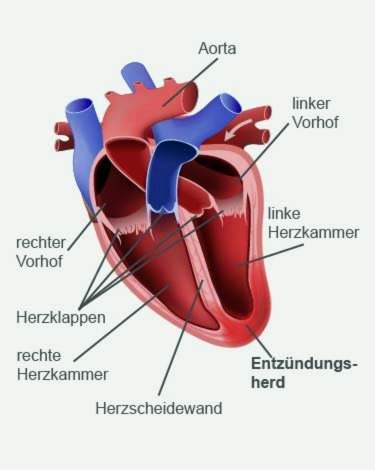
- What is a heart muscle inflammation? Inflammation of the heart muscle cells and usually also of the surrounding tissue as well as the heart-supplying blood vessels (coronary vessels). If the inflammation reaches the pericardium, it is called perimyocarditis.
- symptoms: often no or hardly noticeable symptoms such as increased heart palpitations and heart stumbling; possibly pain in the chest, cardiac arrhythmias and signs of heart failure in advanced myocarditis (such as water retention in the lower legs)
- Trigger: In infectious myocarditis it is pathogens such as viruses (such as cold, flu, herpes, measles or Coxsackie viruses) or bacteria (for example, the causative agent of tonsillitis, scarlet fever, diphtheria or blood poisoning). The non-infectious myocarditis arises, for example, due to faulty immune reactions, radiotherapy or drugs.
- risks: Possible consequences include a diseased enlarged heart muscle (dilated cardiomyopathy) with chronic heart failure and severe cardiac arrhythmia. There is a risk of sudden cardiac death.
- Treatment: V. A. physical protection and bed rest, possibly drugs against the pathogens of infectious myocarditis (such as antibiotics against bacteria); Treatment of complications, e.g. Heart-burdening medicines for heart failure (such as beta-blockers)
- Forecast: With consistent physical protection the myocarditis usually heals without consequences. Otherwise, long-term consequences such as heart failure threaten. Rarely, the heart muscle inflammation ends fatally.
Heart muscle inflammation: symptoms
Heart muscle inflammations are mostly of Viruses or bacteria causes (infectious myocarditis). The symptoms of such an infection are therefore often preceded by myocarditis. These can be, for example, cold and cough, fever, headache and body aches. Join to these flu symptoms increasing Tiredness and exhaustion, weakness,decreasing load capacity or Shortness of breath on exertion, should always be thought of the possibility of infectious myocarditis.
In fact, these symptoms are often the only signs of the onset of acute myocarditis. Symptoms like Appetite and weight loss such as Headache and body aches can be added. Other myocarditis symptoms can be radiating pain be in the neck or shoulders.
If you develop symptoms of heart muscle inflammation days or weeks after a flu infection, you should definitely go to the doctor!
Symptoms in the heart
Usually, a healthy person does not feel his heart. In case of heart muscle inflammation, however, some sufferers notice increased heart palpitations, Some also report one Tightness in the chest (atypical angina pectoris) or of Herzstolpern, This stumbling expresses that the heart comes out of sync again and again:
The heart has a clock on the right atrium. From this so-called sinus node, in a healthy heart, the electrical signals spread evenly across the heart muscle and trigger its contraction. The heart beats coordinated and pumps the blood evenly into the systemic circulation.
When a heart muscle inflammation additional electrical signals or their normal transmission is delayed. Sometimes, the impulses are not even transmitted from the atrium to the chambers (AV block). The normal heart rhythm is consequently disturbed. This can cause some cases of myocarditis palpitations (Tachycardia) or too irregular heart rhythm with dropouts.
Myocarditis: Triggers & Causes
With regard to the causes one distinguishes the infectious from the non-infectious myocarditis.
Infectious myocarditis
Myocarditis is referred to as infectious if it by pathogens is caused. In about 50 percent of cases, these are viral, Infectious myocarditis is often preceded by a common viral infection (cold, flu, diarrheal disease). Especially the so-called Coxsackie B virus is often the trigger of a viral myocarditis. But many other viruses such as the causative agent of herpes, influenza, mumps, rubella or measles can cause heart muscle inflammation.
If viral-induced myocarditis is suspected, the triggering virus will be determined only in exceptional cases. That would have little practical use – there are usually no specific medicines for the virus in question.
Also bacteria can trigger a heart muscle inflammation. Especially in the context of a bacterial blood poisoning (sepsis), in which the heart valves are already affected, the inflammation can also spread to the heart muscle. Typical pathogens here are so-called staphylococci. Another group of bacteria, the streptococcus, can cause heart muscle inflammation. These include, for example, the pathogens of scarlet fever or tonsillitis.
Another bacterial cause of myocarditis may be diphtheria. Rarely, a Lyme disease is to blame for an inflamed heart muscle. Their pathogen, the bacterium Borrelia burgdorferi, is transmitted by a tick bite.
Also rare are fungal infections the trigger of infectious myocarditis: Fungi usually trigger myocarditis only when the patient’s immune system is significantly weakened. This is the case, for example, in the case of AIDS, chemotherapy or the use of immune-suppressing (immunosuppressive) drugs.
Other rare causes of heart muscle inflammation are parasites like the fox tapeworm or unicellular organisms like the causative agents of toxoplasmosis or Chagas’ disease.
Non-infectious myocarditis
In non-infectious myocarditis, no pathogens are the trigger. Instead, the cause is, for example, one Dysregulation of the immune system, The immune system is directed against the body’s own structures, so that so-called autoimmune diseases arise. These include, for example, vascular inflammation, connective tissue inflammation and rheumatic diseases. Such autoimmune diseases can also lead to heart muscle inflammation (autoimmune myocarditis).
Another cause of non-infectious myocarditis is the Irradiation of the thorax as part of radiotherapy for various cancers (such as lung cancer).
Rarely solve drugs a non-infectious myocarditis. These can be, for example, the antibiotics penicillin and ampicillin, the diuretic hydrochlorothiazide and the antihypertensive drug methyldopa.
If you do not find any trigger for the heart muscle inflammation, the doctor speaks of the so-called idiopathic fiddler myocarditis.
Heart muscle inflammation: risks
Inflammation of the heart muscle poses serious dangers – especially if those affected do not spare themselves sufficiently or have a damaged heart. The myocarditis can namely severe cardiac arrhythmias cause. These have significant consequences for the circulation. Because the heart needs the calm, steady rhythm to refill itself with blood after each heartbeat for the next powerful contraction. If it is too fast or irregular due to myocarditis, it can not fill or empty properly. Possible consequence is a Circulatory collapse with sudden cardiac death.
In about every sixth patient, the heart muscle inflammation triggers remodeling in the heart, which ultimately turns into a chronic heart failure lead: The damaged heart muscle cells are converted into scar tissue (fibrosis), the heart cavities (chambers, atria) expand. Doctors speak of this dilated cardiomyopathy, The walls of the abnormally enlarged heart muscle are, so to speak, “blotted out”, so that they can no longer contract with force. So it has developed a permanent heart failure. In severe cases, the pumping power of the heart may collapse completely. It can also be here for sudden cardiac death come.
Heart muscle inflammation: examinations and diagnosis
If you have a suspected heart muscle inflammation, your family doctor or a specialist in cardiology is the right person to contact. If necessary, the doctor will refer you to a hospital for further investigation.
Doctor-patient conversation
The doctor will first talk in detail with you to make your medical history (anamnesis). He inquires about the exact symptoms and whether these may have been preceded by an infection (cold, flu, diarrhea, etc.). In addition, the doctor will ask if you have any underlying medical conditions (especially heart disease) or if you are already having surgery on your heart.
Physical examination
This is followed by an in-depth physical examination. Among other things, the doctor will listen to your heart and lungs with your stethoscope, tap your chest and measure your heart rate and blood pressure. He also looks to see if you show signs of starting heart failure. These include, for example, water retention (edema) in the lower legs.
ECG (Electrocardiography)
Another important study is the measurement of electrical activity of the heart muscle (electrocardiography, ECG). It can detect changes in cardiac activity, as they occur in a heart muscle inflammation. Typical are an accelerated heartbeat (tachycardia) and additional beats (extrasystoles). Also cardiac arrhythmias are possible. Since the deviations usually only occur temporarily, a long-term measurement of cardiac activity (long-term ECG) is advisable – in addition to the usual short-term resting ECG.
cardiac ultrasound
By means of an ultrasound examination of the heart (echocardiography), the doctor can assess the structure and function of the heart muscle. For example, he can detect enlarged heart chambers or a weak pump. Some heart muscle inflammations also accumulate fluid between the pericardium and the heart muscle. Such a Perikarderguss can be detected in the ultrasound.
blood test
Inflammatory levels in the blood (CRP, BSG, leukocytes) indicate if there is inflammation in the body. In addition, heart enzymes such as troponin-T or creatine kinase are determined: they are released from the cells in case of damage to myocardial cells (due to myocarditis, for example) and are then detected in an increased amount in the blood.
If antibodies to certain viruses or bacteria are found in the blood, this indicates a corresponding infection. If the heart muscle inflammation is the result of an autoimmune reaction, appropriate autoantibodies (antibodies against the body’s own structures) can be detected.
roentgen
On the basis of an X-ray of the chest (chest X-ray) can be detected signs of myocarditis-related heart failure. The heart is then enlarged. In addition, a backflow of fluid into the lungs may be visible, due to the weak pumping power of the heart.
Magnetic Resonance Imaging (MRI)
Using magnetic resonance imaging (MRI), the doctor can distinguish inflamed, damaged heart areas from healthy ones. An MRI of the heart is called cardiac MRI.
Tissue removal by means of cardiac catheter
Sometimes heart muscle inflammation also involves cardiac catheterization. A small tissue sample of the heart muscle can be taken (myocardial biopsy). It is examined in the laboratory for inflammatory cells and pathogens.
Heart muscle inflammation: treatment
The treatment of heart muscle inflammation depends on the one hand on the symptoms, on the other hand after the trigger. Physical protection and the treatment of a possible underlying disease represent the cornerstones of myocarditis treatment.
For very severe myocarditis, the patient must be treated in the intensive care unit. There, vital parameters such as heart activity, heart rate, oxygen saturation and blood pressure can be continuously monitored.
Physical conservation
Particularly important in heart muscle inflammation is that the patient is physically completely gentle, This means that he has to avoid any physical exertion, for example in the home. Because a heart muscle inflammation can cause lifelong damage to the heart muscle and the heart valves, if it is further fueled by stress.
Patients with severe myocarditis are hospitalized.
Even weeks after the acute phase of the disease, the patient must not overextend. The doctor decides when a full charge is possible again. As long as there are signs of heart failure, the patient is unable to work. If he relapses prematurely, he risks a relapse and permanent damage.
If myocarditis requires prolonged bed-rest, there is a risk of blood clots forming (thrombosis). For prevention, the patients receive anticoagulants.
Treatment of the cause
The most common causes of infectious myocarditis are viruses. However, there are usually no antiviral drugs available for such viral myocarditis. The treatment here consists essentially of protection and bed rest.
The situation is different with bacterial myocarditis: the doctor prescribes against the causative bacteria antibiotics, Even against other pathogens that cause in rare cases, a heart muscle inflammation, you can usually use targeted drugs. These include antifungals against fungal infections and antiprotozoals against unicellular parasites (such as the causative agents of Chagas disease).
In certain cases, other therapies may be considered for heart muscle inflammation (sometimes only in the context of studies). This can be about the dose of cortisone. It has anti-inflammatory and suppresses the immune system. This may be useful in myocarditis, in which due to a dysregulation of the immune system antibodies to the body’s own structures are formed (autoantibodies).
Treatment of complications
One possible complication of heart muscle inflammation is heart failure, Then the doctor may prescribe various medications, for example ACE inhibitors, AT1 receptor antagonists or beta blockers. They relieve the weak heart. The same thing is done by water-borne drugs (diuretics).
Sometimes the heart beats so irregularly and fast in a myocarditis that is a life-threatening one Arrhythmia as a ventricular tachycardia or ventricular fibrillation threatens. In this case, patients may be temporarily provided with an external shock generator (defibrillator). In the case of ventricular fibrillation, the device automatically emits a strong electrical impulse to restore normal heart rhythm. Fortunately, this measure is rarely necessary.
Did fluid accumulate in the pericardium during myocarditis (pericardial effusion), it should be aspirated with a thin, fine hollow needle (pericardial puncture).
In the worst case, the heart is so severely and permanently damaged in the context of myocarditis that it can no longer maintain its function. Then the patient needs a donor heart (heart transplant).
Heart muscle inflammation: disease course and prognosis
Myocarditis can occur at any age and affect young, healthy people. If the patients take good care of themselves, the course of the disease and prognosis are generally good. Overall, heart muscle inflammation heals in more than 80 percent of cases without leaving lasting damage. This is especially true in viral myocarditis. In some patients harmless extra beats of the heart can then be found in the ECG (electrocardiogram).
The problem with myocarditis is that it sometimes causes little discomfort. Many patients therefore do not spare themselves enough. This is especially noticeable in young people who exercise despite myocarditis. The possible consequences include severe cardiac arrhythmias, which can lead to sudden cardiac death. However, that rarely happens.
Heart muscle inflammation: duration
Acute myocarditis takes on average about six weeks. In individual cases, the duration of the disease depends on the extent of the inflammation and the general health of the patient.
It is also very difficult to tell when a heart muscle inflammation has really healed completely. Even if a sufferer feels well again after overcoming myocarditis, he should spare himself a few weeks and avoid physical exertion. This is the only way to avoid serious late effects (such as heart failure).
Chronic myocarditis
In some patients, myocarditis is chronic. The heart muscle or the ventricle (especially the left side) is dilated (dilated cardiomyopathy). The chamber walls are remarkably thin and can no longer apply the necessary pumping power. Consequently, the heart is limited in its function – it has developed a heart failure (heart failure). Even minor efforts (such as climbing stairs) causes the affected person shortness of breath (dyspnea). The heart failure usually needs to be treated with medication.
Myocarditis: prevention
One can prevent a heart muscle inflammation, by acting against triggering infectious diseases vaccinate and have these vaccinations refreshed as intended. One should follow the recommendations of the Standing Vaccination Commission (STIKO) at the Robert Koch Institute. It is advisable, for example, to vaccinate against diphtheria. This bacterial infectious disease, in addition to the risk of myocarditis, has other dangers such as severe pneumonia. The vaccine is usually given in childhood together with those against tetanus and polio.
Very important, too, is flu To cure infections correctly, For any fever, physical effort should be consistently avoided. The same applies even with a seemingly harmless cold. If you “kidnap” such an infection, the pathogens (viruses or bacteria) can easily spread to the heart and cause heart muscle inflammation.
People who have ever had myocarditis are especially at risk of getting it again (recurrence). You should therefore be extra careful. Above all, the combination of physical stress, stress and alcohol should be avoided. In addition, bacterial skin and mucosal inflammation should be treated early with antibiotics. Such diseases are often the trigger for a renewed Myocarditis.
Additional information
guidelines:
- Guideline “Pediatric Cardiology: Myocarditis in Childhood and Adolescence” of the German Society of Pediatric Cardiology (2012)
Self-help:
- German Heart Foundation